Western Washington University Western Washington University
Western CEDAR Western CEDAR
WWU Honors Program Senior Projects WWU Graduate and Undergraduate Scholarship
Spring 2018
Politics of Reproductive Justice: Planned Parenthood Activism in Politics of Reproductive Justice: Planned Parenthood Activism in
Shades of Blue, Red, and Pink Shades of Blue, Red, and Pink
Sarah Petry
Western Washington University
Follow this and additional works at: https://cedar.wwu.edu/wwu_honors
Part of the Higher Education Commons
Recommended Citation Recommended Citation
Petry, Sarah, "Politics of Reproductive Justice: Planned Parenthood Activism in Shades of Blue, Red, and
Pink" (2018).
WWU Honors Program Senior Projects
. 94.
https://cedar.wwu.edu/wwu_honors/94
This Project is brought to you for free and open access by the WWU Graduate and Undergraduate Scholarship at
Western CEDAR. It has been accepted for inclusion in WWU Honors Program Senior Projects by an authorized
administrator of Western CEDAR. For more information, please contact [email protected].

!
1
Politics of Reproductive Justice:
Planned Parenthood Activism in Shades of Blue, Red, and Pink
SARAH PETRY
Western Washington University
Sociology Senior Thesis, June 2018
In this paper I examine Planned Parenthood’s activism in two politically different states.
Drawing on political opportunity theory and intersectional feminist theory, I question if
and how Planned Parenthood is engaging with issues of intersectionality in these two
states. In addition, I question if they are focusing on issues of reproductive justice, not
only reproductive rights. After conducting semi-structured interviews (N=6), I show that
Planned Parenthood has an increasingly intersectional focus, especially in their coalition
work, and that they are engaging with reproductive justice issues by centering their
patients and considering the multiple barriers that different communities face in
accessing reproductive health care.
Planned Parenthood is a nationally significant provider of women’s health, especially
reproductive care and family planning services. One in five women will receive care at Planned
Parenthood at some point in her life
(PPFA 2018a). In particular, Planned Parenthood health
centers serve many vulnerable
1
populations: poor women, women living in rural areas, women of
color. Planned Parenthood’s patients are primarily individuals who face various oppressive
structures of race, class, sex, and gender, all of which impact their ability to access and receive
quality health care – both reproductive and otherwise.
Since the 2016 election, Planned Parenthood has constantly been fighting against anti-
choice policies pushed forward by the Republican controlled national legislature and White
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
1
The Affordable Care Act (2010) describes “vulnerable” populations as those that are racial and
ethnic minorities, homeless, incarcerated, and/or veterans.

!
2
House
2
. Legislators in Washington, D.C., are determined to strip Planned Parenthood’s federal
funding
3
and delegitimize the organization. In states across the country, other Republican
legislators are working to erode Planned Parenthood’s funding
4
, forcing the closure of health
clinics that serve populations who might otherwise have no access to health services for
hundreds of miles, and seeking to control women’s bodies, especially regarding their very
personal and vital reproductive health and choices.
Because Planned Parenthood clinics serve predominately women, who are more likely to
be poor, more likely to experience the negative health effects of lived racism and sexism, who
have historically been denied the reproductive control over their own bodies that Planned
Parenthood offers, proponents of Planned Parenthood argue that it is of vital importance that
these clinics stay open (PPFA 2017). Without Planned Parenthood clinics, women from rural
areas, for example, are less likely to be able to access health care, less likely to have access to
birth control, and more likely to have unwanted pregnancies that they must bear to term. As
such, Planned Parenthood Action Fund (PPAF), the political arm of Planned Parenthood, lobbies
the legislature, does electoral work, and advocates for their patients to ensure that those patients,
who rely on Planned Parenthood health centers for medically necessary care, can continue to
access those clinics and the services they provide (PPAF 2018). After the 2016 election, PPAF
adopted the motto “These Doors Stay Open”, promising to the public, to the people they serve, to
continue to provide health care to those who need it the most and who, without Planned
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
2
For example, the current administration is attempting to remake the Title X program, which
“provides preventive health care to those most in need”, enabling low-income women to access
birth control, STD tests, cancer screenings, and regular check ups. (PPAF 2018)
3
Planned Parenthood receives funding from the federal government, but they cannot use those
funds for abortion services, which are the services that the administration opposes.
4
For example, in Iowa, the legislature passed a bill that blocks Planned Parenthood from
receiving grant funds that help them provide accurate sex-education to Iowan youth.

!
3
Parenthood, might not have it at all (PPAF 2018). PPAF’s actions, because of their political
nature, deeply affect women’s access to care and, often, their lives more generally
5
.
Planned Parenthood Federation and Action Fund both serve as social movement
organizations (SMOs) in contemporary feminist movements
6
. Historically, Planned Parenthood
focused on issues that were representative of certain feminist ideologies and certain gendered
bodies. Specifically, Planned Parenthood focused on reproductive rights, such as the right to use
birth control, without also recognizing the structures (race, class, location, etc.) that limited
women’s access to birth control – legal or not. In this paper I examine PPAF’s health activism to
determine if Planned Parenthood is engaging with issues of intersectionality in two politically
different states. Specifically, I ask is Planned Parenthood engaging with issues of
intersectionality? And, if so, how are they doing this in two politically different states? Finally,
is Planned Parenthood centering reproductive justice?
These questions are significant because Planned Parenthood primarily serves women
whose daily experiences of being raced, classed, sexed, and gendered impact the way in which
they can and do receive care (Krieger and Smith 2004). In addition, certain women have more
agency, “autonomy plus options”, to decide if, when, and how to reproduce (Showden 2011).
Poor women, women living in rural areas, women of color, LGBTQ+ individuals, all face
structures (laws, norms, physical space) that limit their agency and their control over their own
bodies (Loyd 2014). These women also face histories of oppression, especially in regards to their
reproductive rights (Threadcraft 2016). I will determine if Planned Parenthood, in serving these
women, is attentive to that intersectionality, to the multiple layers of identity and politics that
oppress certain women’s reproductive choices and marginalize certain bodies. This goes beyond
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
5
Planned Parenthood is often a provider of life-saving care, especially through their STD and
cancer screening services, sex education, and treatment of various STDs (PPFA 2017).
6
SMOs are organizations whose mission aligns with that of a certain social movement.!

!
4
simply access to health care. These issues include providing access to safe housing, the ability to
leave abusive partners, the ability to keep and raise the children they do have without
succumbing to poverty or homelessness, the ability, generally, to exercise their civil rights in
their reproductive health and daily lives.
The second question
7
is particularly relevant today, at a time when political polarization
is heightened and when the two major parties have adopted oppositional stances on abortion:
pro-life (anti-abortion rights) and pro-choice (pro-abortion rights). Planned Parenthood is
especially vulnerable to attack and defunding in conservative (red) states, such as Missouri
8
, yet
in progressive (blue) states, such as Vermont, Planned Parenthood is well respected and
politically influential. Because of these differences in position, I analyzed Planned Parenthood’s
work in both a sympathetic and a hostile state – one red, one blue, from the same region of the
United States. In doing so, I determined how this political difference impacted Planned
Parenthood’s ability to engage and their actual engagement with intersectionality.
Finally, reproductive rights have been the center of many recent debates. Often, these
debates take the form that the national parties have: pro-life and pro-choice. But reproductive
health is far more complicated than pregnancy or abortion. While abortion is an issue in the
reproductive justice movement, it is not the whole story. Women have faced many other barriers
to their own reproductive choices: forced sterilization, lack of access to accurate sex-education,
lack of access to birth control, and more. Reproductive justice, then, includes reproductive rights
but also requires consideration of the other factors impacting access to reproductive health care
and individual’s ability to make decisions about their reproductive health. Because of Planned
Parenthood’s historical focus on rights, and their national image as an abortion provider (even
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
7
How does Planned Parenthood engage with intersectionality in two politically different states?
8
On May 10, 2018, the Missouri legislature voted to cut off Medicaid funding to Planned
Parenthood, which prevents Medicaid patients from receiving care at Planned Parenthood.!
!
5
though only 3-6% of their services are abortion related), I question if they can go beyond that
dominant narrative and bring issues of reproductive justice “from margin to center” (hooks
2000). I use this language of margins for two reasons. The first is that large SMOs and white
feminists “ignored the existence of all non-white women and poor white women” in their earlier
activism and advocacy, such that those groups were on the margins of feminist activity (hooks
2000:2). The second is that many issues of reproductive justice impact marginalized groups,
“[those] who are daily beaten down, mentally, physically, and spiritually – [those] who are
powerless to change their condition in life” (hooks 2000:1). To center these marginalized issues
and groups, then, is to focus on those issues, those people, and make reproductive justice the core
of an organization’s work and focus.
This case study is small and set in a specific location, but my findings are illustrative of
Planned Parenthood as a whole. Planned Parenthood health clinics serve vulnerable populations
nationwide, primarily women, who experience physical and emotional effects of intersectional
oppression. Is PPAF, the political arm of Planned Parenthood, pursuing politics that will serve
these patients – both in Planned Parenthood clinics and in their daily lives? How does the
political environment impact that engagement? Is Planned Parenthood centering reproductive
justice?
In this paper I begin with a brief history of feminist movements, paying particular
attention to Planned Parenthood’s evolving role within those movements. Next, I review
literature on the different ways scholars have engaged with social movements and how their
findings support my research questions. I then include a section on organizational composition,
this is primarily because Planned Parenthood has three main and deeply interrelated purposes:
health care, education, and advocacy. I focus primarily on advocacy in this paper, but in places

!
6
address the other purposes when they connect with advocacy. Then I describe my data and
methods, followed by an in-depth analysis of my findings. Finally, I draw conclusions and offer
directions for future research.
FEMINIST MOVEMENTS AND PLANNED PARENTHOOD
Planned Parenthood has been active in various feminist movements and campaigns since
it was founded more than 100 years ago. They are one large SMO situated in a long history of
feminism, and my questions, in particular, are grounded in that feminist history and evolution
9
.
In the early and mid 20
th
century, Planned Parenthood focused on establishing clinics and
providing accurate reproductive health care and education (PPFA 2018a). In the 1960s and early
1970s, Planned Parenthood began, along with many other feminists and women’s health
organizations, to focus on fighting for and providing political access to safe and legal abortions.
During this time, women’s health activists framed abortion as issues of rights and agency (Loyd
2014). White women – largely of the middle- and upper-classes – wanted control over their own
bodies, advocating for their right to choose if, when, and how to have children (Loyd 2014). In
1973, with the Court’s decision in Roe v. Wade, these women won a significant battle for
reproductive rights and choice
10
.
However, while Roe was upheld as victory of choice, a victory for women’s agency, it
was less so for poor women and women of color. Poor women, particularly poor women of
color, were “subject to coercive reproductive policies enacted directly on their bodies through
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
9
Intersectional feminism, which informs my questions, is a relatively new iteration of feminism
that has gained popularity in academia and public life in recent years. It offers a critique of other
feminist movements, as well as possibilities for more diverse and representative feminist activity,
both in the actions of organizations such as Planned Parenthood, and in individual actions.
10
Roe v. Wade (1973) is a Supreme Court case that extended the right to privacy to include a
woman’s right to have an abortion. It is regarded as the case that legalized abortion.

!
7
surgical procedures and the welfare system” (Loyd 2014:155). These policies included forced
sterilization, lack of access to safe abortions geographically and economically, and other
constraints for those dependent on the paternalistic welfare system. Women, particularly women
of color, began organizing in response to forced sterilization in the 1960s. Thus, while Roe
signified the right for women to choose to abort pregnancies, Relf v. Weinberger (1977) signified
the right for women to choose to have pregnancies
11
. Together, these two cases brought national
attention to the ways in which women’s bodies had been controlled by health care providers and
the welfare system, and they substantively extended agency to women in their own reproductive
health
12
.
These two distinct cases demonstrate the diversity of reproductive issues. Today, as in the
late 20
th
century, feminists are not always concerned about the same oppressive policies and
systems and thus do not always fight for the same causes. As white, elite women came to
feminism, they created a feminist movement that was based in their own experiences of sexual
oppression. Because women are moved to become feminists based on their own experiences
first, the various white, elite feminist movements neglected to attend to the experiences of
women who have different experiences of gender, class, sexuality, and race (Ahmed 2017). In
omitting these groups, this particular feminism suited white, elite women’s specific interests and
experiences (Reger 2017).
Because white women, along with the largely white feminist organizations they
constructed and run, were more visible in the media, their activism and successes were typically
prominently displayed and celebrated. The organizations they constructed, such as National
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
11
The Relf sisters, age 12 and 14, were both intentionally sterilized at a federally funded clinic in
Alabama without their consent. They won their case, Relf v. Weinberger (1977), before the
Supreme Court, legally ending the practice of forced sterilization.
12
This extension was limited, though, and forced sterilizations, for example, continued after Relf,
though at lower numbers (Loyd 2014).

!
8
Organization for Women (NOW), National Abortion Rights Action League (NARAL), and
Planned Parenthood Federation of America (PPFA), represented these particular feminists – both
in their leadership and in their goals. This was, to some degree, precipitated by the demographic
makeup of the cities where these groups had offices (Reger 2012). Groups today have the
potential to be more attentive to, in particular, racial and ethnic diversity when they maintain an
ideology of inclusion as well as structural opportunity for leadership by women of color (Scott
2005). However, there is little evidence to suggest that racially diverse leadership necessarily
leads to changes in policy orientations and goals of those groups (Reger 2012).
By examining Planned Parenthood in two states, each diverse in unique ways, I explore if
this organization falls into the same patterns of past iterations, and if it diverges by engaging
with issues of intersectionality. Simply being aware of the diversity of their patients does not
indicate that an organization is centering those patients, people of color or LGBTQ+ individuals,
for example. However, in analyzing how this organization succeeds and fails to include non-
white, non-elite leaders and patients, I seek to reveal if and how they engage with
intersectionality and whether they are centering reproductive justice in that work.
LITERATURE REVIEW & THEORETICAL FRAMEWORK
Planned Parenthood, in particular PPAF, is a large and influential SMO in the feminist
movement today. However, because they are often targets of attack and misinformation
campaigns, this organization is difficult to access for academic research
13
. But researchers often
study feminism as practice, or as a social movement, through examinations of SMOs – many of
which are similar to PPAF in their composition and goals. Reger and Staggenborg (2006), for
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
13
Planned Parenthood was recently the target of a misinformation campaign that stated that they
were selling fetal tissue in order to fund their services. This was incorrect, but (temporarily)
damaged the organization’s image and legitimacy.
!
9
example, study NOW leadership, tactics, and success through in-depth interviews with
organizers and activists. Research on SMOs demonstrates the ways in which organizational
strategies, tactics, goals, and ideologies shift in response to changing political opportunity
structures, as well as the broader social and economic context (Harnois 2012; Reger 2002). In
addition, research on SMOs can illuminate changes in the underlying movement.
Specifically, although many feminist movements had focused some energy towards the
acquisition of and protection of reproductive rights, the reproductive justice movement did not
emerge until the 1990s. Planned Parenthood, previously an SMO in the women’s movement,
broadly, adopted a place within the reproductive justice movement. Black women at the United
Nations International Conference on Population and Development coined the term “reproductive
justice” in 1994, and the movement itself originated shortly thereafter (Staggenborg and
Skoczylas 2017). The language of reproductive justice is often conflated with the abortion rights
movement, even though, as identified previously, these are not the same (Loyd 2014). As the
feminist movement progressed, women of color pushed for the more inclusive language of
reproductive justice, rather than abortion rights, to attend to women’s diverse reproductive
experiences based on their social and economic positions (Threadcraft 2016). As evidenced by
the evolution of movements for reproductive rights in the 20
th
century, the naming and
subsequent movement for reproductive justice has continued to broaden (Staggenborg and
Skoczylas 2017). The justice framing “led by women of color, strives to make explicit
intersectional connections to other struggles, linking reproductive rights to human rights
agendas” (Staggenborg and Skoczylas 2017:220). If Planned Parenthood is centering
reproductive justice, they are also making these connections, recognizing that reproductive rights
are intertwined with many other rights and issues.

!
10
The reproductive justice movement emerged at a time of relatively many political
opportunities
14
. Political opportunity refers, generally, to the “features of the political
environment that influence movement emergence and success” (Staggenborg 2011). Meyer
(2015) argues that social movements are episodic because these political features or structures
vary over time and space. Movements tend to grow when there are “greater political openings”
that enable activists to organize and mobilize safely and with the possibility for success (Meyer
2015: 39). These openings are not fixed and may be available to only certain organizations.
Planned Parenthood regularly has greater political opportunities in progressive (blue) states,
while typically facing constraints in conservative (red) states. This difference enables me to
examine how Planned Parenthood engages with issues of intersectionality in the face of two
different political opportunity structures, and to see to what extent this theory explains Planned
Parenthood’s activism.
According to Meyer (2015), “social movement organizations form to coordinate the
process of turning inchoate grievances into issues and apathy or dissatisfaction into political
action” (45). SMOs, then, are often the actors in social movements with the resources necessary
both to identify political opportunities and to respond with appropriate strategies and tactics.
SMOs, though, have varying structure based on the type, size, and ideology of the organization
(Ganz 2000; Staggenborg 1988). These different structures are oriented toward different
strengths and weaknesses, different tactical repertoires, and different levels of success and
longevity (Freeman 1973; Staggenborg 1988, 1989; Taylor 1989; Ganz 2000). Organizations
differ on two primary dimensions: level of formalization and level of centralization (Staggenborg
1988, 1989; Freeman 1973). More formalized SMOs have established decision-making and
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
14
!For example,!Bill and Hillary Clinton, both strong supporters of Planned Parenthood and
reproductive rights, were in the White House, offering more opportunity for Planned Parenthood
to engage in proactive political action.!
!
11
operational procedures, a division of labor by function, membership criteria, and formal rules
governing subunits (Staggenborg 1989). Formalized SMOs, in particular, are able to maintain
movement activity when faced with a lack of political opportunities (Taylor 1989; Meyer 2015).
In addition, formalized SMOs tend to have leaders who can offer institutional knowledge of
strategies and tactics, as well as maintain relationships with legislators or coalition partners, so
that the organization is able to respond when moments of greater opportunity arise. Planned
Parenthood is highly formalized, with many different levels and functions, and is able to
maintain that institutional knowledge, respond to changing political opportunities, and maintain
coalitions over time.
Coalitions are significant in helping organizations participate in collective action as well
as in creating networks of influence to maximize success. Coalitions typically form between
groups with similar interests, but there are no guarantees of successful formation or activism
(Staggenborg 1986). Coalition formation and sustainability is more likely between formalized
SMOs because these SMOs have professional staff able to act as organizational representatives
to coordinate and maintain coalition work (Staggenborg 1989). In addition, formalized SMOs are
able to pursue coalition work in one area, while using other resources to pursue their other tactics
or goals (Staggenborg 1986; Taylor 1989; Ganz 2000). Staggenborg (1986) argues that coalitions
typically form either to take advantage of opportunities and resources or to respond to threats. In
addition, the chances that a coalition will be successful depend on the likelihood of reaching a
victory. When victory is likely, “resources tend to be plentiful and organizational maintenance is
not threatened; consequently, shared goals are more salient than organizational maintenance
needs” (Staggenborg 1986:380). Planned Parenthood, in part because of its age and
institutionalism, has many coalition partners who share common ideology and goals. In
!
12
conservative states, these coalitions are especially important because resources for progressive
organizations, generally, are more limited and Planned Parenthood is able to build coalitions to
better use those resources and pursue their goals.
Today, reproductive justice activists, learning from past movements, “struggle with
building a diverse and inclusive movement, and they work in organizations and agencies founded
in the 1970s and 1980s geared at women’s lives” (Reger 2017). These feminist struggles appear
at different levels, and feminists find success in different ways. In those organizations founded in
earlier generations, these struggles happen at the individual and institutional level – redefining
and muddling categories (Butler 1990), breaking down walls and barriers (Ahmed 2017), and,
often, failing to incorporate diverse voices and intersectional ideology (Reger 2017). My first
research question, is Planned Parenthood engaging with issues of intersectionality, is designed
to look at how Planned Parenthood is engaged with this common feminist struggle.
Feminist theory has evolved over time in many different iterations, that sometimes
oppose and other times complement each other. Although the idea that feminism is the
movement for equality of women and men was popularized in the 1960s, many feminists have
critiqued this definition (e.g. Brown 1992; hooks 2000). Instead, “Feminism as a movement to
end sexist oppression directs our attention to systems of domination and the interrelatedness of
sex, race, and class oppression” (hooks 2000:33). Intersectional feminist theory, then, focuses on
the ways in which power functions to create identities and structures of oppression. Sara Ahmed
(2017) proposes that reflecting on how certain bodies are not accommodated by a world can
illuminate the consequences of our intersectional identities. Bodies that are differentially raced,
gendered, and classed experience various power structures based on the interaction and
convergence of those bodily experiences. Intersectional feminist theory involves examining the
!
13
ways in which various identity categories intersect to create structures of dominance and
privilege, and serves as a resource for studying the dynamics of power on bodies.
Kimberlé Crenshaw (1991) proposes, “identity groups in which we find ourselves are in
fact coalitions” (1299). As such, attending to “multiple dimensions of privilege and difference is
necessary to develop awareness about a whole spectrum of subordinated histories and struggles”
(Cho, Crenshaw, and McCall 2013:801). This knowledge can enable SMOs to form broad
coalitions, based in these diverse and often shared experiences of subjugation. Broad coalitions
then can serve as a form of intersectional politics, which dismantle “structures that selectively
impose vulnerability upon certain bodies” (Cho et al. 2013:803). Subsequently, broad coalitions
might offer a way “to dismantle the world that is built to accommodate only some bodies”
(Ahmed 2017:14). Planned Parenthood is part of many coalitions, some of which are a form of
intersectional politics; others are built to respond to a need or to achieve a specific goal.
The reproductive justice movement incorporates many of the earlier SMOs involved in
women’s and health activism. Planned Parenthood, as well as the various political and
educational arms of this organization, is one such organization that claims a place in the
reproductive justice movement. In this paper I will answer: is Planned Parenthood engaging
with issues of intersectionality? If so, how are they doing this in two politically different states?
Is Planned Parenthood centering reproductive justice? In doing this, I hope to offer a broad
analysis of an organization that is both an essential health care provider and a powerful and
important feminist SMO.
!
14
ORGANIZATIONAL COMPOSITION AND STRUCTURE
Margaret Sanger founded the first birth control clinic in the U.S. in 1916. This formed the
foundation of her later activism, as she opened the Birth Control Clinical Research Bureau and
incorporated the American Birth Control League both in 1923. These two organizations later
merged and became PPFA (PPFA 2018a).
There are a few important distinctions to make between the various arms of Planned
Parenthood. The first is the difference between Planned Parenthood Federation of America
(PPFA) and Planned Parenthood Action Fund (PPAF). While both are non-profit organizations,
PPFA is a 501(c)(3) organization and PPAF is a 501(c)(4) organization. 501(c)(3) organizations
are broadly defined as charitable organizations, while 501(c)(4) organizations are commonly
defined as social welfare organizations (IRS 2018).
Because PPFA, in these early iterations, was primarily focused on providing health care
and education, it was classified as a 501(c)(3) organization. Because of this, PPFA was (and is)
limited in what and how much political activities it can conduct. PPFA may participate in some
lobbying, so long as it is not a “substantial part” of their overall activities. In addition, PPFA may
not participate – directly or indirectly – in any campaign on behalf of any candidate for elective
public office (IRS 2018). In line with these requirements, PPFA’s mission states:
Planned Parenthood works to educate and empower communities, provide quality health
care, lead the reproductive rights movement, and advance global health. Planned
Parenthood believes sexual and reproductive health rights are basic rights. (PPFA 2018b)
This mission includes political advocacy, but it is not a substantial part of the overall activities.
PPFA, then, is primarily focused on reproductive health care and education.
When Faye Wattleton, the first woman of color to be president of PPFA, founded PPAF
in 1989 she did so with the intent that it be the political advocacy arm, engaging “in political
!
15
education campaigns, grassroots organizing, and legislative and electoral activity” (PPFA
2018b). She knew Planned Parenthood would have to be more political in order to keep its doors
open and provide care. Therefore, PPAF is classified as a 501(c)(4) organization so that it can
pursue lobbying as its primary activity to further social welfare without jeopardizing its tax-
exempt status. In addition, PPAF may engage in some political campaigns, so long as that is not
its primary activity (IRS 2018). As such, PPAF’s mission is:
To protect informed individual choices regarding reproductive health care, to advocate
for public policies that guarantee the right to choice, as well as full and non-
discriminatory access to reproductive health care, and to foster and preserve a social and
political climate favorable to the exercise of reproductive choice. (PPFA 2017)
Today, as in 1989 when PPAF was founded, it is focused on protecting access to reproductive
care and choice. These three aims – health care, education, and advocacy – are foundational to
Planned Parenthood’s various bodies and complement one another at local, state, national, and
international levels.
There are both 501(c)(3) and (c)(4) organizations represented in this study. Any affiliate
of PPFA is a (c)(3); similarly, any affiliate of PPAF is a (c)(4). In this study, I examine one
regional affiliate of PPAF, as well as two local affiliates of PPFA within that same region. There
are two national PPFA offices (one in New York, the other in D.C.) and 56 affiliates of Planned
Parenthood, at least one in each state. In addition, there are more than 650 local Planned
Parenthood health centers nationwide. PPAF has regional, state, and local affiliates. The regional
affiliates typically have different staff for each state in that region. In addition, local affiliates are
primarily present in large states, such as California. In analyzing this data I will be very clear
about which organization type and level I am referring to.
!
16
DATA AND METHODS
In this study I use data from in-depth interviews (N=6) that I conducted from February
through May 2018. These interviews were with two current (at the time of the interviews)
Planned Parenthood Action Fund (PPAF) employees, and four past Planned Parenthood
Federation of America (PPFA) and PPAF employees. In addition to this data, I relied on archival
data from organizational websites and tax histories. Together, this data enabled me to answer my
research questions: is Planned Parenthood engaging with issues of intersectionality? How are
they doing this in two politically different states? Is Planned Parenthood centering reproductive
justice?
I used two key contacts, one past activist and one current activist (at the time of the
study), who were able to each give me access to additional interviewees. This snowball
technique was necessary and became intentional because Planned Parenthood, generally, is a
difficult organization to access. In particular, this is because of the strong and often violent
countermovement activity that directly targets their organizations and activists. Emails from
unknown sources are often phishing scams from opponents seeking to attack Planned
Parenthood. As a result, in my initial recruitment emails I only received one positive response.
That response was from an activist in a state that is friendly to Planned Parenthood, both in the
legislature and in the culture more generally. From branches in other states, where Planned
Parenthood faces more attacks – both physical and otherwise – I received only negative or non-
responses to requests for interviews.
Because of the organizational concern to maintain security for patients and activists, I
used snowball sampling and increased anonymity measures. Using the two key contacts I
developed, I was able to expand the scope of my study to examine the consequences of political
!
17
differences in the coalition work, goals, and successes of different branches of Planned
Parenthood. The two key contacts I facilitated were a current activist from a (blue) state with
great political opportunities and sympathy for PPAF’s work, and a past activist who worked in a
(red) state with few political opportunities and often hostility for both PPFA’s an PPAF’s work.
After obtaining contact with my initial sample, I conducted in-depth interviews with each
of the subjects I identified through my snowball sample. The respondents I sought were from
politically different states (red, blue), and those from the past were from the same general time
period. The red state in my analysis has a Republican governor and there is a Republican
supermajority (greater than 80%) in both the state House and Senate. In addition, in the last
legislative session two pieces of anti-abortion legislation were proposed, which directly target
Planned Parenthood and impact their ability to provide this service. The red state is also
conservative, both in terms of their politics and legislation. In the blue state, the governor is a
Democrat, there is a Democratic majority (greater than 50%) in both the state House and Senate,
and there have been no negative bills targeting Planned Parenthood proposed in the past
legislative session. The blue state is generally more progressive in their politics and legislation.
The past activists worked during the Bush and Obama administrations, both of which
were generally more supportive of Planned Parenthood’s mission (the latter substantially more
so). The current activists, at the time of the interview, were working within the scope of a
Republican dominated national legislature and a Republican presidency. I chose these two
national moments and selection of red and blue states for their distinct political differences
(political opportunity opposed to political constraints), and the ways in which those differences
at the national level impacted state and local level Planned Parenthood activism and functioning.
!
18
Interview questions addressed the nature of the activist’s participation in the organization,
strategies and tactics, issues, and goals and successes of organizational activities (see Appendix
A). While their mission speaks to reproductive justice by incorporating language of racial and
economic justice, I used in-depth interviews to see if they are actually engaging with these issues
at the state and local level, and how individuals within the organization understand and seek to
further that cause. In addition, each interviewee had a unique view of the social world, and that
context added depth and meaning to their responses. Finally, I conducted interviews because
they “bring human agency to the center of movement analysis” (Klandermans and Staggenborg
2002). As such, my analysis is grounded in each respondent’s language and personal
understanding of the issues at hand.
Because of the limited size and scope of my interview sample (N=6), I supplement this
data with archival reports. In particular, I examined tax data (IRS Tax Form 990), recent
organizational financial reports, and website data (both past and present). These documents are
all publically available and provided information on the organization structure of PPFA and
PPAF, and current and past organizational activities and events (see Appendix B). Together, this
data assisted my analysis of the structural barriers Planned Parenthood faces and the changes the
organization has made over time, as well as supplemented my interview data where interviewees
could not recall specifics about events or legislation. I recognize that the six individuals I
interviewed are not a representative sample of activists or branches of PPFA or PPAF. However,
these activists and the issues they address are illustrative of the larger national context.
In compiling my data, I identified patterns, differences, and changes over time. In
particular, I looked at the differences between organizational activities in red and blue states, and
at times of high and low political opportunities. I also looked at how issues of reproductive care
!
19
and reproductive justice have changed over time. My analysis is centered on how Planned
Parenthood has shifted their focus from reproductive rights more narrowly to reproductive justice
more broadly, and what political barriers and aids enable or deter these shifts in two different
states.
ANALYSIS
Our work this session, we could describe it as being like, ‘drawing a pink line around [the
state]’, and defending our state from whatever nonsense the federal government tries to
throw at us. (Current PPAF Public Affairs Manager, Blue State)
We have to celebrate those small victories to be able to keep morale up and kind of see
the progress that we’re making. (Current PPAF Public Affairs Manager, Red State)
The political environments in these two states are vastly different. The current PPAF
Public Affairs Manager from the blue state (Blue PAM; for descriptions of each interviewee see
Appendix C) reflected on the defensive, resistance work they’re doing at a national level, but
also noted the strong state-level support for Planned Parenthood that enables her office to engage
in this national work because they’re not facing attacks within the state. Instead, she uses her
resources to pass proactive legislation to expand women’s access to birth control and to protect
residents from actions of the national government. In the red state, though, the current PPAF
Public Affairs Manager (Red PAM) faces a hostile legislature that constantly seeks to undermine
Planned Parenthood’s work and limit access to abortions and other essential care. In this state,
getting proactive legislation even proposed is a time-consuming and often futile goal. Instead,
she focuses her energy on fighting against state legislation that would negatively impact Planned
Parenthood, women, and other marginalized groups.
In my analysis, I focus primarily on Planned Parenthood’s advocacy, because it is in their
advocacy work that I can see political patterns and changes over time. The past activists framed
!
20
issues of health care and education within a very different political moment than those currently
working for PPAF, resulting in different forms of advocacy and different focuses in that work. In
addition, Planned Parenthood serves patients in their health clinics who face intersectional
structures of oppression, but I’m curious to determine if and how they engage with those issues
in their political advocacy. Similarly, only at (c)(4) Planned Parenthood offices (i.e. Action
Fund) can that advocacy work be a substantial portion of their overall activities. So I
intentionally selected my sample, being primarily from PPAF affiliates, in order to see how these
advocates deal with intersectionality in their legislative and political work.
Purpose: Providing Health Care
The purpose of an affiliate offers the blueprint for their activism. In Red Past 1’s PPFA
office, the main purpose was to provide health care. Doing so was at the center of the advocacy
work she did as a community organizer. Similarly, Blue PAM noted that the purpose for her
state-level PPAF affiliate was,
To advocate for our mission in advancing reproductive health rights and justice locally,
and then regionally and nationally as applicable. So our main focus is to ensure that
voters are aware and acting upon those issues.
Health care, then, in the blue state is still centered, but they do this through engaging voters on
issues of health policy. Meanwhile, in the red state, Red PAM articulated the purpose of her
position slightly differently.
Definitely to try to, you know we have that long-term goal of breaking the supermajority
in [this state]. I’m also there as a stopgap between an extremely hostile legislature and
their efforts to try and close the doors of our health centers in [this state]. So, I’m there
both to advocate for and lobby for good policy and stop bad policy, and also, at the same
time, get friendlier folks elected so that we don’t have to spend so much time and energy
fighting against bad policy.
She is also focused on health care, but she expresses this focus by preventing politicians from
trying to “close the doors” of Planned Parenthood clinics. She has to spend much of her time

!
21
fighting against these attacks, so the purpose in the red state is far more defensive than
proactive
15
. Red Past 2 said the purpose of the state-level PPAF office he directed was, simply,
“to avoid negative legislation”. This is very similar to Red PAM’s remarks about constantly
being on the defensive. In a red state, Planned Parenthood has to focus on health care by
defending it, rather than increasing and supporting it.
Blue Past 1, who worked only for PPFA, focused on health care in her description of its
purpose.
To provide health care for people who needed it, with a focus on reproductive health
care… Keeping people healthy and serving low-income or marginalized people who
don’t have access elsewhere [to healthcare].
This aligns well with the national PPFA purpose and is appropriate for the (c)(3) status of the
office she worked for. In addition, she spoke specifically to the patients that Planned Parenthood
serves, “low-income or marginalized people” who rely on Planned Parenthood health centers for
their health care – reproductive and otherwise. These patients are often those receiving Title X
funds, who are on Medicaid or other public insurance, or individuals who cannot access care at
other locations for a variety of reasons. Her remarks are neither proactive nor defensive, but
speak more to the actual day-to-day work of Planned Parenthood health centers nationwide.
In addition, both Red Past 1 and Red Past 2 noted that when they worked for PPFA their
purpose was to serve patients. Red Past 2 told a story about getting a patient across state lines to
access an abortion, which was not technically a responsibility of a field organizer, but he knew
she was poor, and would not otherwise be able to get the care she needed. He concluded by
noting that the purpose of his affiliate was always “to get people care when they needed it.”
These interviews revealed that PPFA prioritizes the provision of health care to their patients –
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
15
I describe the two different types of advocacy work as “proactive” and “defensive” because
that is the language that all my interviewees used.
!
22
both in red states and blue states. In red states the stakes for centering patients are higher, and
might include crossing state lines, providing care for free, or accompanying patients to local
hospitals to advocate for them there. But each of the activists I interviewed spoke to the essential
nature of this work.
It is because of these different political environments that I ask both, is Planned
Parenthood engaging with issues of intersectionality? And how are they doing this in two
politically different states? The political differences greatly impact what goals PPAF sets, as well
as the extent to which PPAF pursues those goals to reach success. To answer these interrelated
questions about intersectionality and political opportunity, I draw on and interpret the language
and examples my interview subjects offered. Similarly, to answer my third question, is Planned
Parenthood centering reproductive justice, I analyze and interpret the importance of the various
stories that each of my interviewees shared with me.
Evidence of Intersectionality
Planned Parenthood is attending to intersectionality in a few ways in their advocacy
work. As evidenced with interview and archival data, Planned Parenthood forms coalitions with
other progressive groups, whose interest is not necessarily women’s health, to further goals
beyond reproductive health care. In addition, they focus on issues and bills that will impact their
patients in a variety of ways, in and out of Planed Parenthood health centers. Finally, underlying
each of these moves, Planned Parenthood is centering patients. They raise up patients’ stories
and experiences, considering how their activism, their work, impacts their patients and how to
serve these communities.
In each of these areas, Planned Parenthood is, at some level, engaging with questions of
intersectionality. As noted below, Planned Parenthood looks at intersectionality in terms of how
!
23
gender and race, or gender and class, or gender, race, and class intersect to impact their patients
and others in their states. They consider questions of gender normativity and heteronormativity,
and they seek to expand the categories included in “women’s health” to attend to these various
intersectional identities, questions, and needs. In Table 1, I consolidate this evidence of
intersectionality in terms of Planned Parenthood’s coalition partners, the issues they engage with,
and their work to center their patients.
Table 1. Evidence of Intersectionality.
Intersectionality
Coalitions
Issues and Goals
Centering Patients
Broad
Focused on various structures
that impose intersectional
oppression
Diverse
Issues ranging from trans
rights, to immigrant rights, to
equal pay, and more
Intentional
Building trust and listening to
determine the needs of the
communities they serve
Coalition partners. In their coalition work, Planned Parenthood is attentive to the various
ways in which gender intersects with other aspects of identity to constrain and impact bodies.
Red PAM noted that “If there is a social justice or progressive organization in [our state] we try
to work with them, because, again, pooling our power is the best way we can create change in
such a conservative state.” Thus, by forming coalitions, Planned Parenthood is able to pool
scarce resources rather than competing for them. Red PAM offered a specific example, their
coalition with Add the Words, “an organization that’s been working to update [the state’s] non-
discrimination legislation to include sexual-orientation and gender identity so that gay and trans
[residents] cannot get fired or lose their housing for being gay or transgender.” Red PAM
proposed that, though it is challenging to pursue this goal, the organizations work together so
they continue to make slow progress.
!
24
I’m not gonna not work on Add the Words, that’s just a near and dear and personal issue
for me and so that’s always going to be on my list of goals because its something that I
see as a need in the community, but I know that that’s gonna be a long-term goal…
because I am aware of the political realities of the state. (Emphasis hers)
She has to be attentive to the political responsiveness to an issue regarding LGBTQ+ rights, and
recognizes that this won’t change overnight. But by maintaining a coalition with Add the Words,
the issue remains salient in the progressive circles in this state. It is something that, while PPAF
cannot dedicate too many resources to this coalition, they can assist, as they are able, to create
change in the long term.
This particular long-term coalition with Add the Words is an example of Planned
Parenthood’s engagement with intersectionality, particularly regarding questions of gender
normativity and heteronormativity. Specifically, by doing this work, they are able to consider
how gender normativity impacts their patients and people in this state. In engaging with these
questions and this coalition, PPAF can better attend to the needs of LGBTQ+ individuals in their
advocacy, as well as in their health care and education programs. By acknowledging the ways in
which gender normativity functions to constrain certain bodies, Planned Parenthood is better able
consider how gender and sexuality intersect to marginalize certain communities and then to
center those communities’ needs and their stories in their advocacy.
By contrast, in the blue state, Blue PAM described far more diverse coalition partners,
with interests ranging from women’s health to voting rights to homelessness. One example she
offered was their work with “Mom’s Rising and the Economic Opportunity Institute… we’re
standing in solidarity and support with them so we’re trying to pass equal pay across [the state].”
She noted, “We are proud coalition partners with many, many different organizations. So it
really just kind of depends on time of day and what campaign we’re doing.” This comment
demonstrates the political openness to progressive causes: there are many progressive
!
25
organizations in this state, many with a focus that complements PPAF’s, and resources are less
scarce and can be shared more easily among more groups. In addition, working with multiple
partners enables PPAF in this state to pursue goals beyond reproductive health, goals that are
deeply tied to reproductive justice issues, but less explicitly so.
Many of the activists, both present and past, mentioned women’s rights groups as
common coalition partners. Blue PAM said, “We’re also almost all the time aligned with
different women’s rights groups. Like, kind of our usual folks that we’re always hanging out
with, like Legal Voice or NARAL, and so on.” These coalitions are “usual” in that PPAF has
been partnering with these organizations for much of their history and they work together
because of their similarities in missions and composition. However, most activists mentioned
these groups almost as an afterthought, typically following a list of other, more diverse
organizations. This indicates that as PPAF has expanded their mission they are actively working
to engage with wide-ranging issues that involve questions of intersectionality. By expanding
their coalition partners, PPAF is able to expand their focus and to consider additional
intersectional questions and structures, to see what changes are needed – in policy, health care,
education, and in the organization itself – to respond to their coalition partner’s interests and
needs. But they maintain these older coalitions in part because their missions are so deeply
interrelated and in part so they can also share resources with more groups.
In both red and blue states, deciding what organizations to form coalitions with is a
matter of finding organizations whose mission aligns with that of Planned Parenthood. However,
as previously mentioned, PPAF has expanded their mission and, as a result, has expanded the
criteria for coalition partners. In the red state, PPAF has diverse coalition partners, but they have
to be careful in how “loud and proud” they are about some of these. Red PAM noted that the
!
26
limited resources for progressive causes and constant attacks directed at Planned Parenthood
limits their overt coalition work.
Everybody has competing interests, and yet also a shared interest, but you have to come
at that shared interest with your organization’s best interests in mind… You know, it’s
just a lot of competing interests and there’s – it’s not like [our coalition partners are]
doing anything wrong, they’re doing things that are in their organization’s best interest.
This quiet and careful coalition work speaks to Planned Parenthood’s need, in red states, to
protect their image and, at least publically, work for their mission more narrowly.
Unlike in blue states, in red states PPAF has to be more careful about how they do this
work. This is largely because, in red states, PPAF has to preserve their resources and influence to
fight to strict anti-woman, anti-choice legislation that they face every legislative season. But, as
Red PAM told me, they do form coalitions with conservation groups, immigrants rights groups,
and more. They may have be quiet, but PPAF is still making a concerted effort to engage with
issues regarding how environmental concerns intersect with gender, issues regarding how race
and gender intersect, and issues that examine even more complex relationships between politics,
policy, and bodies. In addition, as Red PAM said, they come to coalitions with their best interests
in mind. By building these coalitions, even ones invisible to the public, PPAF is acting in their
best interest: expanding their mission and scope to engage with issues of intersectionality,
expanding their advocacy and centering those communities they already serve in their health
centers.
PPAF’s dedication to coalition work, even in the face of political hostility, demonstrates
their recognition of the importance of this work in following their mission. Red Past 1 noted that,
because many other progressive organizations are facing the same political environment, they
pool their resources. She spoke about a “bill that would’ve targeted or would have made it illegal
to text while driving” that could have enabled racial profiling. At first glance, PPAF’s opposition

!
27
to a texting bill seems far afield from their mission. Yet, in that case, they used their volunteers
to help block this legislation because they understood that that bill would have impacted certain
bodies, black and brown bodies, and further threatened already vulnerable populations
16
. This
example demonstrates PPAF’s engagement with issues of the intersection of race, immigration
status, and gender in their coalition work. Specifically, they can acknowledge that racism enacted
through racial profiling has significant health impacts
17
, and can directly impact individuals’
ability to access health care and live healthy lives.
This mutual relationship, of sharing volunteers and knowledge, is at the core of coalition
work. Although every progressive organization faces some level of insecurity and hostility in the
red state, they cooperate, sharing what they can and helping, as they’re able – even if they have
to be silent partners. This dedication to work together on issues beyond the many bills attacking
abortion rights is in part due to personal convictions, such as Red PAM’s dedication to Add the
Words, but also due to a recognition that any attack on civil rights is an attack on health care and
health more broadly.
In blue states, PPAF is also attentive to which organizations share their mission and
focus. Blue PAM described their current focus and how it impacts coalition building.
We care really deeply about pursuing reproductive justice and racial equity. So
increasingly, we’re endeavoring to do more to prioritize people of color led and centered
organizations in our work, that’s one of our priorities.
This focus on racial equality is evidenced on PPAF’s websites – both at the national- and state-
level. In their 2016-2017 Financial Report
(Planned Parenthood 2017), Planned Parenthood
affirms what Blue PAM noted.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
16
!She spoke particularly about immigrant populations in her description of who would be at risk.
17
These health impacts include greater levels of stress, leading to clogged arteries and early
death.
!
28
Planned Parenthood continued to build and strengthen relationships across movements to
protect access to health care with a deeper commitment to elevating the intersections of
reproductive health, rights, justice, and other issues affecting the communities we serve.
Planned Parenthood believes everyone should have access to health care, no matter what
– but far too often, systemic barriers, including the harmful legacies of oppression and
white supremacy, stand in the way of achieving health equity for all. Full access to health
care starts with strong, healthy, and supported communities.
This declaration, along with Blue PAM’s comments, could be empty. However, the coalitions I
described offer evidence of this work and attention to intersectional and structural impediments
to health care access in the communities they serve in red states, blue states, and nationwide.
Planned Parenthood is intentionally seeking coalition partners who represent the
communities they serve in their health centers. They recognize that supporting these
communities is necessary in order to protect their access to health care and their self-
determination. They do this by partnering with groups such as LGBTQ+ organizations and racial
justice organizations, whose members know the needs of the communities they represent.
Planned Parenthood can then assist these groups while also learning from the very people they
serve how to do this work better. They attend to the various structures that limit access to health
care based on the intersections of, for example, race and gender, and seek to deconstruct those
structures by engaging in coalition work.
Issues and goals. In part because of the time of year during which I conducted interviews,
the current activists spoke primarily about electoral work. When I conducted my interviews, the
legislative session in the red state had recently concluded, and Red PAM was engaged in
electoral season, in preparation for primaries in early May. Similarly, when I interviewed Blue
PAM, her legislative season was wrapping up, with only a week and a half left in the legislative
session. She was focused on that, while also looking ahead to the electoral season that would
begin for her as soon as the legislators adjourned. The past activists spoke more to legislative
!
29
work, but together, their work during these two seasons demonstrates Planned Parenthood’s
relationship to public policy.
Blue PAM offered a long list of legislative items that PPAF had brought to the legislature
or was supporting in the legislature. Some of these were directly related to the central purpose of
providing reproductive health care, while others were not. She described one significant package
during the legislative season.
One of our priorities was the Voting Justice Legislation that has been going through,
there’s four different bills. One is a Voting Rights Act, which has to do with basically
helping cities to enact districted elections so that city council members, for example,
can’t just all be at large; they have to be more representative of more areas of the city –
coming from different parts of the city. There’s also automatic voter registration, which
has to deal with, instead of you opting in to get registered to vote when you get your
license, it’s just an opt out. Same day voter registration or extending the period within
which you can register to vote, and then pre-registration for 16 and 17 year olds. So that
whole package is making good progress, but we’re looking to coalition partners to let us
know – the ones who are really the leads on it – to let us know if it’s in trouble or
anything like that and we chime in when we can.
This Voting Justice Legislation was a priority, but, as she mentioned, PPAF was not taking the
lead on that. Their coalition partners are taking the lead, but, because PPAF has more resources
and political recognition in the blue state, she can lend resources and aid as necessary. This
legislation is not directly related to health care, but it is related to health policy and civil rights.
Specifically, the voting rights portion would guarantee more direct representation of
communities on city councils. This potentially protects politically marginalized groups,
especially from smaller neighborhoods or poor neighborhoods that often lack representation, and
gives them more voice on city councils. This encourages self-determination and provides a
platform for increased political participation from disenfranchised and marginalized populations.
Similarly, the various voter registration portions – automatic registration, same-day
registration, and pre-registration – would likely increase voter turnout and political participation.
!
30
Removing barriers to voting is essential for increasing participation and policy engagement.
Planned Parenthood serves these marginalized communities in their health centers, which
increases their agency in deciding when and how to receive health care. By increasing these
patients’ access to politics, these bills would also increase their agency in their political lives.
Given PPAF’s ability to propose legislation and devote resources to issues beyond abortion and
birth control, they can focus on issues that are related and deeply impact how marginalized
groups engage in politics.
However, because PPAF’s mission is “To provide women’s health and reproductive
choice through advocacy”, this state-level branch is also engaged with legislation that impacts
women’s health. Blue PAM described the Reproductive Parity Act, which deeply impacts
reproductive health.
The Reproductive Parity Act, that’s one of our top pieces of legislation, we’ve been
working on it for at least like 5 years. That would mandate that all insurance plans in [this
state] cover abortion care along with a broadened range of contraception. Instead of a
plan saying, like, ‘oh, you can only have this one kind of birth control’, saying all FDA
approved methods should be approved without a copay.
The Reproductive Parity Act is more obviously related to PPAF’s mission. However, it is a
broadly pro-choice piece of legislation. I say “broadly” to distinguish this bill from the strictly
pro-abortion bills that the activists from the red state lauded as victories (although, really, these
victories tended to be defeats of anti-abortion legislation). This bill does protect a woman’s right
to access an abortion, expanding that right to make it more accessible to women with limited
income or substandard insurance coverage, but it also increases access to more diverse forms of
birth control. Some women cannot use certain forms, and some women simply prefer certain
forms of birth control. This legislation would protect women’s right to make that choice with
their doctor and would guarantee coverage. This extends the birth control provision of the ACA,
!
31
a victory that several of the past activists I interviewed held up as a momentous victory for
women’s health and women’s rights.
The Reproductive Parity Act, in its breadth, is another example of Planned Parenthood’s
consideration of intersectional needs. In particular, by advocating that insurance plans cover
abortions, PPAF recognizes that abortion access is limited by economic standing. Women who
are from the middle and upper classes might be able to afford an abortion, even without
insurance, but women from lower classes, women who are more likely to seek abortions, are less
likely to be able to afford them. Similarly, by requiring insurance coverage for all forms of FDA
approved birth control women would be able to make unconstrained choices about their
reproductive health. This increases women’s agency immensely, making every birth control
choice – including abortion – a viable option for women.
In addition to this more strictly women’s health bill, Blue PAM mentioned the
Reproductive Health Access For All Act, which did not make it out of committee this year.
That bill would have been kind of similar to the Reproductive Parity Act, but it would
have been far more inclusive, because it also would have included things like STD
screening testing and treatment and counseling, and breast feeding support and services,
and gender affirming hormone therapy for trans individuals, and would also include
coverage for undocumented immigrants, and so we’re really disappointed that it didn’t go
further this year. It would do more and be more inclusive for all, but it’s gonna be a huge
priority next year.
As she says, this bill would have expanded access to many varied reproductive health services.
The various components demonstrate different ways in which reproductive health care can be
different for different bodies. For example, the provision for hormone therapy for trans
individuals demonstrates recognition that trans rights are reproductive rights, and that PPAF is
attentive to how gender identity and sexual orientation intersect to marginalize trans individuals.
In addition, this provision demonstrates that PPAF is committed to dismantling “structures that
!
32
selectively impose vulnerability upon certain bodies”, in this case, trans bodies (Cho et al.
2013:803).
While Planned Parenthood has historically focused on women’s rights, with a narrow
definition of women, Blue PAM spoke to their focus on non-heteronormative gender and sexual
identities and rights. Similarly, Planned Parenthood health clinics serve undocumented
immigrants, individuals who otherwise would not be able to access health care, and the provision
providing coverage to undocumented immigrants suggests that Planned Parenthood is trying to
serve this population both in its health centers and in the legislature. Specifically, this group is
entirely disenfranchised from the voting process in the United States, so PPAF, along with
various other SMOs, are able to help move this group from margin to center, raising up their
voices and focusing on their needs in their legislative work. Their dedication to this bill, with it’s
many provisions demonstrate Planned Parenthood’s dedication to their diverse patients, patients
who experience marginalization based on their various identities: sexual orientation, race,
immigration status, and more.
Centering patients. Planned Parenthood clinics are the main vehicles for providing health
care, but they also incorporate health education and advocacy. For example, several interview
subjects described the Health Center Advocacy Program. The HCAP involves “[talking] with
patients and find out a) how we can better serve them but also b) how we can better let them
know what’s happening in their communities” (Red PAM). It is a chance for PPAF activists to
“talk with people face-to-face about the public policy issues that are happening that could impact
their ability to even be in that waiting room” (Blue PAM). The HCAP is a way for Planned
Parenthood health centers to determine their patients’ health care needs, to educate and inform
patients about policy issues, as well as bring patients stories into their advocacy work. By doing
!
33
this work, PPAF can begin to see how the intersections of race and gender, for example, impact
health care and how policies impact different raced and gendered bodies.
Because Planned Parenthood clinics serve vulnerable populations, I was curious how
PPAF attends to the needs of these diverse populations and various barriers to health care in their
advocacy work.
I think probably the biggest way that we [attend to the diverse population in our state] is
by trying to be increasingly centered around our patients, because we know that we are
not truly meeting our mission if our patients, and their needs and concerns, are not being
lifted up first and foremost. We know that they are representative, often, of some of the
most marginalized populations in the state, and they come from all walks of life, of
course. For those who see us the most regularly, we’re often the only health care provider
they ever see and so they’ve become the people we want to center. (Blue PAM)
Centering patients is essential work for an organization such as Planned Parenthood because
their patients are precisely those communities that face “systemic barriers, including the harmful
legacies of oppression and white supremacy” (PPFA 2017) and those communities that are the
most politically and socially marginalized. In order to center patients, PPAF implemented the
HCAP program, which enables Planned Parenthood, as an SMO with political legitimacy, to
deploy their political influence to amplify the voices of their patients and center their needs in
their advocacy work.
Giving legislators these stories can demonstrate how the policies they pass can impact
their constituents in deeply personal ways. For example, Red Past 1 mentioned that she spoke to
a patient in reference to bill that allowed doctors to deny patients based on religious reasons. The
patient had been experiencing a lot of bleeding after giving birth, which can be life-threatening.
And she was bleeding, and she was given a prescription, and the health care provider
called the Walgreen’s to fill that prescription… Anyway, so this woman could not get her
prescription filled at Walgreen’s because the person there said, ‘I can’t do this for
religious reasons’… So the woman had to actually go to an alternate pharmacist and get
that filled. And that was a life-threatening event. So, she could have died.

!
34
This story drew attention to a flaw in a law that was designed to protect religious beliefs and
practice but had deeply negative consequences for this woman. And this story was just one
example. Red Past 1 went on to describe how the existing law also enabled pharmacists or
doctors to refuse to treat HIV positive patients, because they believe that HIV is God’s
punishment for being gay. So overturning this law benefitted not only women seeking life-saving
care or women seeking a Morning After Pill
18
, it also benefitted many LGBTQ+ people, as well
as women who might contract HIV from positive partners. Although the bill, on the surface, is
intended to protect religious belief – such as preventing a pharmacist from filling a prescription
they believe will lead to an abortion, when they believe abortion is wrong for religious reasons –
these stories, from women, from gay men, from patients, reveal how detrimental such a law can
be to certain bodies, especially those who are gendered and sexed in particular ways.
Planned Parenthood uses HCAP to bridge the gap between health care and policy by
sharing stories, such as this one, to demonstrate how lawmaker’s impact their constituents’ lives
and bodies through the legislation they push and pass. PPAF center patients’ stories in their
advocacy, recognizing that Planned Parenthood exists, at the most fundamental level, to provide
care to those patients – at health clinics, through educational programs, and through advocacy.
In line with this work, Red PAM spoke to her personal commitment to Add the Words. In
forming a coalition with Add the Words, PPAF is able to attend to the distinct structures that
limit LGBTQ+ individual’s ability to access health care. PPAF is becoming increasingly
attentive to issues impacting this community, both through specific bills, such as the religious
protection bill mentioned above, but also through coalition work with government agencies.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
18
Red Past 1 noted that people in “very conservative places consider the Morning After Pill to be
abortion, too… even though its not because its preventing a pregnancy. So, the definition of a
pregnancy is a fertilized egg that’s implanted into the uterine wall, and the Plan B or the Morning
After Pill prevent implantation, so its not technically pregnancy.”
!
35
We partner with different agencies within the Department of Health and Welfare to help
– you know, right now we’re working on a program to better serve the LGBTQ
population in Idaho specifically for intimate partner violence, because we’ve noticed that
there’s a huge gap in services in our communities for intimate partner violence
specifically with the LGBTQ community. (Red PAM)
LGBTQ+ individuals lack full citizenship protections in this state and, as a result, have less
access and ability to leave violent partnerships. In addition, they also have less access to hospital
care, less access to the legal system, and face many other barriers to health care. This is tied to
the history of health discrimination against LGBTQ+ individuals (e.g. Gould 2012). While the
state de-legitimizes the experiences of LGBTQ+ individuals through non-recognition and by
providing few, incomplete resources for this group, Planned Parenthood, a major provider for
LGBTQ+ communities, shares their stories and brings their experiences to the center of their
advocacy. In addition, these stories demonstrate what services are lacking – such as intimate
partner violence intervention and assistance – and can help PPAF determine what the needs are
of the communities they are trying to serve and center.
To serve LGBTQ+ individuals, immigrants, and other vulnerable populations, Planned
Parenthood must “[assess] the needs of the community and [respond] to those” (Red PAM).
Although PPAF cannot focus all their energy on the communities they serve simultaneously,
especially in a red state where they face constant attacks they face from the legislature and
hostility from the public at large, they recognize that these populations are their patients and
those who face oppression and intolerance in such a conservative state. Because “Planned
Parenthood is part of the web of services”, especially for medically underserved and medically
vulnerable populations, they center their patients, tell their stories, and build trust to determine
what those communities need (Blue Past 1).

!
36
Similarly, in the blue state, Blue PAM noted that they are increasingly “endeavoring to
do more to prioritize people of color led and centered organizations in our work.” By prioritizing
these relationships, PPAF can cooperate with those groups to determine the needs of
communities that might distrust Planned Parenthood because of their history and national image.
In addition, by building coalitions with racial justice or immigrant rights groups, for example,
PPAF has greater opportunity to understand and engage more with the intersectionality of those
issues with reproductive rights and reproductive justice. Both of these branches appear to be
moving forward with intention and attention to their mission.
In doing this, though, PPAF has to build trust in these communities. Even though
individuals from these politically and socially marginalized communities are Planned Parenthood
patients, they are likely to be untrusting of PPAF because of that marginalization and Planned
Parenthood’s history of elite leadership and action. In the red state, for example, Red PAM noted
that the way they pursue their mission varies based on location.
The communities that we serve look a little different based on where those health centers
are located… [We have to determine] how we can best serve [each] community and how
we can begin to build trust… So how we can kind of begin to make those steps to build
trust within those communities to even begin the process of understanding what their
needs are.
Because each health center serves, typically, a specific city or area, the patients are different
based on the community in that specific place. To make sure that they are representing and
serving those patients, they have to build trust and use their existing tactics
19
to provide the best
service possible. In addition, they don’t assume to know what is best or what the needs of any
given community are. Instead, they center patients’ and communities’ voices to understand what
each community needs and how to serve them.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
19
HCAP is an example of this.
!
37
This action, of centering patients, centering communities, is very similar to how Planned
Parenthood health center’s center patients. As Blue Past 1 noted, “helping people get healthy,
and decide how they get there” is a priority of the (c)(3) side of Planned Parenthood. The (c)(4)
side, then, can enable and reinforce this goal by advocating for patients and for communities,
centering their stories and their experiences in their legislative work and lobbying to help create
the changes that these communities need.
Planned Parenthood, both in their health centers and in their advocacy work, is engaging
with broad and intersectional issues. This is visible in their broad coalition work: by intentionally
pursing coalition work with organizations whose focus is on racial justice, LGBTQ+ rights, and
more, Planned Parenthood is able to more deeply consider how race and gender, for example,
intersect to create certain structures of oppression. Because many of their patients are people of
color, these coalitions offer a way for Planned Parenthood to help dismantle those structures and
serve their patients better. In addition, their focus on issues, such as the Reproductive Parity Act,
demonstrates that they can see how reproductive health care has historically been one of those
selectively oppressive systems. For example, by advocating for insurance coverage of hormone
therapy they are recognizing that hormone therapy is and should be included in reproductive
health, as well as questioning heteronormativity in health care and policy. Finally, in their work
to center their patients, Planned Parenthood is better able to see the specific needs of the
communities they serve. Together, through coalition work, engaging with diverse issues and
legislation, and centering their patients, Planned Parenthood is engaging with issues of
intersectionality and working to dismantle various systems that create intersectional oppression.
!
38
Political Opportunity: Limits on Intersectionality
We live in state that’s very hostile to Planned Parenthood. We live in a state that’s very
intolerant of the communities that we serve, both if you look at race, if you look at gender
identity, if you look at sexual orientation. (Red PAM)
We could get someone here in [this state] to do a speech on the floor about how
important funding for abortion is, even including like a male moderate democrat. (Blue
Past 2)
In a red state, with a Republican-dominated state legislature, PPAF is constantly working
defensively. Red PAM mentioned that breaking the “supermajority” in her state was a critical
long-term goal, as this would enable PPAF to pursue proactive legislation and focus fewer
resources on defense. Meanwhile, in a blue state, with a Democratic majority in the state
legislature, PPAF is able to pass proactive legislation. Even here, though, Blue PAM told me that
they endorse and assist additional candidates who are supportive of Planned Parenthood. These
candidates who are “pro-women’s health”, as Blue PAM described them, offer additional
supporters in the state legislature, helping PPAF to solidify Planned Parenthood’s presence there.
No matter where, Planned Parenthood is always in search of more sympathetic legislators to
protect their cause and work in the legislature.
Table 2. Intersectionality and Political Opportunity.
Intersectionality and Political Opportunity
Blue State
Red State
Successes
Proactive
Passing new, broad, proactive
legislation that benefits their patients
and the communities they serve
Defensive
Preventing negative legislation that
would chip away at reproductive rights
already in place
Barriers
Few
Sympathetic legislature, public support
Many
Hostile legislature, complicated
legislative process, public distrust
!
39
To begin my analysis of political openness, I examine the goals that each activist
highlighted alongside how they then defined success. I then describe and analyze a particular
bill, the Twelve Months of Birth Control bill, that passed through both states legislatures to
describe the different barriers to success that exist in each state. In Table 2 (above) I summarize
these political differences and consequences.
Personal and political successes. Interestingly, every person I interviewed who used to
work in any capacity in the red state (Red Past 1, Red Past 2, and Blue Past 2, who did some
regional and interstate work) mentioned the same significant bill. This state, like many others in
the post-Roe years, tried to limit women’s access to abortion by proposing a trans-vaginal
ultrasound bill. Red Past 2, who worked for PPAF through 2009, noted that the precursor to this
bill “was a silly ultrasound bill that would have forced women to pay for an ultrasound, whether
they wanted it or not, but if they were seeking an abortion they had to have it.” This bill would
have limited access to abortions especially based on economic factors, because women who
could not afford to pay for an ultrasound would be forced to carry the fetus to term. However, if
a woman cannot afford an ultrasound, it is unlikely that she has the economic capacity to afford a
child, so this could create a cycle of poverty and dependence. PPAF defeated that bill, but later,
when Red Past 1 was working for PPAF, the legislature attempted to increase abortion
restrictions again.
They tried to pass a trans-vaginal ultrasound bill. So, instead of like regular ultrasounds,
which most states require before you can have an abortion, they were trying to force this
intra-vaginal ultrasound, where you shove a wand up the woman’s vagina and do an
ultrasound that way because they erroneously believed that you could get better – like
you were more likely to hear a heartbeat and like all this stuff – which they think that a
woman magically hearing the heartbeat of a fetus inside of her was gonna trigger all of
her mothering hormones and she would not have an abortion.

!
40
This bill called for medically unnecessary treatment, under the guise of increasing the likelihood
of hearing a fetus’ heartbeat. As this activist argues, this bill was not designed to increase the
health of women seeking abortion; rather, it was designed to deter them from getting an abortion.
To defeat this bill, PPAF implemented a national media strategy. Blue Past 2, who served
as the Communications Coordinator for this region during the time, spoke to her role in defeating
the trans vaginal ultrasound bill as a success she was very proud of. The national media strategy
proved effective, as Red Past 1 mentioned, when legislators who she never would have been able
to communicate with in the past reached out to her to discuss this bill. These legislators were
from rural areas of the state, they were legislators that PPAF lobbyists could never get meetings
with
20
, yet they reached out to Planned Parenthood offices to ask whether or not trans vaginal
ultrasounds were medically necessary and to seek counseling on the specifics of the bill showing
that the organization is a trusted women’s health expert. Bringing national attention to the
invasive and medically unnecessary nature of trans vaginal ultrasounds increased public feelings
of anger and gained the attention of legislators, making them “panicked” (Red Past 1).
Defeating this bill benefitted all women, but Red Past 1 said that defeating this bill
specifically benefitted rape victims.
[Defeating that bill benefitted] rape victims and those who have encountered any kind of
sexual assault, or anybody who is just not as open with their body. I mean, having
something stuck up inside you, in a very invasive way can be very re-traumatizing to
people or be just straight up traumatizing to those people who aren’t comfortable with
that when there is a perfectly viable alternate option that is external and just as reliable
and much safer… But really it benefits every woman in the state. It costs more money to
do an intra-vaginal, its more invasive, there are more options for infection that way, I
mean, its unnecessary on every single level. So it saves you money, and inconvenience,
and potential harm.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
20
Red Past 1 told me that some legislators would cancel meetings with her right before they
were supposed to start, and some simply wouldn’t show up at all.
!
41
This paralleled some of what Blue Past 1 said, about their successes being focused on their
patients and increasing individuals agency in their own health care. It also protects women from
experiencing additional harm, unnecessary harm, and gives them greater ability to make
informed and non-coerced decisions about whether to get an abortion.
These successes, in the legislature and in health centers, directly impact women’s
reproductive agency and health. As Blue PAM said, simply, these various successes benefit “our
patients.” This patient-centered advocacy is visible in their health care provision and health care
policy work, but it is also apparent in their electoral work. For example, Red PAM described one
meaningful electoral success.
We endorsed the first Latina city council member to ever run for city council [in a certain
city] and we were able to help her get elected last fall and that was another huge success
for us that we were really excited for and proud of… I think the communities that we
serve benefitted most from that success because its so important to have that
representation, and they’ve never had a Latina person – or a Latino person, a Latinx
person – on [that] city council.
Even in their electoral work, PPAF is focused on increasing representation of the communities
they serve, their patients. This is similar to Blue PAM’s comments about being “increasingly
centered around our patients, because we know that we are not truly meeting our mission if our
patients, and their needs and concerns, are not being lifted up first and foremost.” In their
advocacy work, in their educational programs, and in their health centers, Planned Parenthood is
focused on their patients.
Although many of PPAF’s successes in the red state were defensive, they did have some
proactive victories in the legislature and in electoral work by forming coalitions with other
progressive organizations to push more diverse agendas. Their success in helping to elect the
first Latinx representative, as previously mentioned, is one example of this proactive work.
Progressive organizations in this red state are all constrained by the unsympathetic legislature
!
42
and, often, hostile populace. However, by engaging in coalition work on certain campaigns, they
can each expand their scope and their influence on policy. With few progressive organizations,
and little political space and support for those organizations and the causes they represent, the
ones that survive must work together to sustain themselves and their work. It seems that the
larger, more professionalized progressive organizations are the most likely to survive and form
coalitions in the red state. With limited resources, the formalized structure enables these groups
to maintain movement activity in spite of a hostile political environment. Because of this
necessity to come together in coalition work, these organizations are somewhat intertwined: their
success depends on their ability to form coalitions and secure necessary resources.
Barriers to success: twelve months of birth control. PPAF and PPFA, overall, each have
different approaches to serving Planned Parenthood patients. In addition, each state faces
different barriers and constraints and has different ways of reaching their goals and defining
success. There was one bill that was common between the two states, that almost every person I
interviewed mentioned: the Twelve Months of Birth Control bill. Both state legislatures worked
with some version of this bill, but the results in each state demonstrate how different these
political environments are.
In the red state, the process for proposing legislation is highly complicated, and adds an
additional barrier to PPAF’s ability to propose proactive legislation, such as Twelve Months of
Birth Control. Red Past 1 described the legislative process as one of the biggest barriers they
faced in achieving their goals.
A big barrier for us [here] is that if we ever want to pass a piece of proactive legislation,
[the legislature] has what’s called a pink slip process… So, if you want to propose a piece
of legislation, it gets what is called a ‘pink slip’. It does not get a bill number
automatically. It goes to this one committee, and they decide if they’re even gonna allow
it to become a bill. And, and of course [that committee] is stacked and they always vote
no on our issues. So our proactive legislation rarely ever can become a bill.
!
43
Red PAM also noted this process as a barrier. Conservative politicians opposed to Planned
Parenthood’s activism dominate the single committee that decides if pink slips become bills. So
when proposing legislation, such as the Twelve Months of Birth Control bill, Red PAM has to
make long-term plans. She noted, “I’ve got a multi-year plan to try and get Twelve Months of
Birth Control passed.”
The first step is to get the bill passed out of the pink slip committee. Red PAM described
her goal for Twelve Months of Birth Control this legislative season:
We just wanted to get a print hearing this year, and we were able to not only get a print
hearing but also get a public hearing. Now that’s a huge win for us. It didn’t pass out of
committee, it failed in the public hearing, but that was more than what our goal originally
was and we have to celebrate those small victories to be able to keep morale up and kind
of see the progress that we’re making.
This small victory – going beyond the goal they had set – was a major success for PPAF in this
red state. Meanwhile, Blue PAM faced far fewer barriers in passing the same bill.
Well, just last legislative session we passed a bill, the Twelve Months of Birth Control
bill, saying that, I mean, it’s pretty straightforward but also a huge impact, saying that a
provider, an insurance company, should (not a provider, but an insurance company) they
should cover 12 months of contraception at a time. So, if a woman goes to her family
planning provider and gets a prescription, she can go to the pharmacist and get all 12
months of pills right there.
Instead of the multiyear, long-term plans that Red PAM has to work with in order to get a
“straightforward” bill even proposed, Blue PAM passed it in one session.
Both, though, celebrated their victories, big and small. Blue PAM offered a story to
demonstrate the significance of this bill.
It might sound just like, ‘Oh, that’s convenient, cool.’ But at the same time, there’s also,
like, real hardships that many women face in getting to the pharmacy. So, for example,
one of my favorite volunteers, when she was younger, she didn’t have a car, she had this
rusty bicycle that she got at a garage sale; she worked shift work and would have to
scramble down the road to get a new pack of pills every month. And also she had a
doctor who was a total jerk who misinformed her and she though that she had to go back
to him for a prescription every month, which is absolutely appalling and wrong… We
!
44
also have the hard data to back it up because if you’re on Medicaid family planning that
already happens, so the state already has the data to show that when you can give patients
all their contraceptive for the year all at once, they don’t miss pills as often and the
pregnancy, the unintended pregnancy rates go down.
This is another example of Planned Parenthood’s focus on their patients. This woman faced
many barriers to accessing birth control: economic hardship, inadequate transportation, and false
information from a trusted medical professional. This woman’s story is not exceptional. Many
other women face similar barriers, and many have fewer resources to overcome those barriers.
PPAF centered this story, but also backed it up with data: providing women with access to 12
months of birth control at a time decreases unintended pregnancy rates, which, in turn, decreases
abortion rates. Comparing the same bill in these two states demonstrates how the political
environment impacts not only Planned Parenthood, but also women in each of these states. In the
blue state, passing this bill was much easier than in the red state, where they have had to create a
multi-year plan to pass it.
Other barriers. There are many barriers to serving vulnerable populations in every state.
This is partially due to the lack of access and trust, as well as lack of resources to serve their
needs and focus these communities. Red PAM spoke to the constant challenges to secure
necessary resources.
Resources are finite and, especially under this current administration, they become more
scarce, and so we’ve had to become more creative and we’ve had to make cuts
unfortunately in places that we haven’t wanted to, and try and utilize other resource in
was that, you know, things like our volunteer teams and try and lean on people to help
with things that we haven’t had to in the past.
Being “creative” might mean building new coalitions, such as one Red PAM described with a
refugee rights group in her state, or increasing their volunteer base so they have more people
who can do work in more areas. It also might mean “making sure our candidate questionnaires
have racial justice questions on them, you know, to make sure that we have candidates whose
!
45
goals and ideal match our mission” (Red PAM). PPAF uses questionnaires across the country to
determine whether or not to endorse candidates in elections at every level. In this red state, in
particular, they have made specific changes to make sure that every candidate they endorse is
supportive of women’s health and racial justice, two issues that politicians in this state are less
likely to affirm than in the blue state. However, they refuse to endorse candidates who don’t earn
a perfect score on that questionnaire, because those candidates are not entirely supportive of
Planned Parenthood’s mission.
In spite of various barriers to intersectional focus and work, Planned Parenthood is
insistent in pursuing and expanding their mission with their patients at the forefront of that work.
Whether their successes are proactive or defensive, PPAF considers whom they are serving and
how proposed and enacted legislation will impact those communities. Although it is more
difficult to propose legislation in red states, PPAF works in coalitions with other groups, pooling
their resources to fight or promote legislation. In addition, they are attentive to how legislation
that seems simple might impact different bodies, different communities. This is clear in their
work to pass the 12 months of birth control bill, which would benefit women, generally, but also
certain women, specifically poorer women and women who lack access to health care.
Reproductive Justice
Planned Parenthood is working to center reproductive justice in their advocacy work.
Reproductive justice requires consideration of the many factors impacting access to reproductive
health care and individual’s ability to make decisions about their reproductive health. Focusing
on these diverse issues is much more challenging in a red state than in a blue state. In the blue
state from my study, PPAF has made conscious efforts to expand their focus and work with more
diverse groups. They advocate for issues beyond reproductive rights, issues such as trans rights,
!
46
employment opportunity and equal pay, and immigrant rights. Similarly, in the red state PPAF
works in coalitions with refugee rights groups, immigrant rights groups, and LGBTQ+ rights
groups. In addition, they have made changes to their candidate questionnaire with the intention to
endorse and support candidates who are not only pro-women’s health, but are also engaged with
issues of racial justice.
These moves indicate a change in Planned Parenthood’s underlying mission and strategic
plan. They also suggest that the organization has recognized their history of white elitism and
focus on reproductive rights, narrowly, and is intentionally seeking to make changes that will
move the organization in a new direction. This work, then, is clearly being done at the
institutional level and in particular through changes in their mission and how they pursue it.
Stories, advocacy, and policy. Each activist I interviewed told me stories. All of these
stories, at some level, in some way, were about their patients. By telling stories in this way, each
activist illuminated the very real ways that policy – both proactive, such as Twelve Months of
Birth Control bill, and negative, such as the Trans-Vaginal Ultrasound bill – impact their patients
ability to make healthy decisions, their ability to exercise control over their own bodies, and their
daily lives. Blue PAM noted that “[We do] a lot of sharing stories and putting our patients at the
center of that. So, lifting up their experiences and putting it into a relief of real life and that these
are people in your district that you represent.”
I included many of those stories throughout this analysis, in part because there were
many – Red Past 1, alone, told me more than 10 stories about patients and activists – but also
because each activist I interviewed told these stories with intent, recognizing the sacred nature
storytelling. Politicians and physicians too often ignore women’s and marginalized individual’s
stories. But these stories reveal how policy impacts bodies and agency. In addition, these stories
!
47
can illuminate the intersectional ways that policies impact different patients, different bodies.
One able-bodied poor woman with a bike might be able to access birth control each month.
Another might not. And the consequences of that inequality are visible in bodies and in stories.
Planned Parenthood appears to be making a concerted effort to center stories, storytelling,
and listening. In their HCAP program, Action Forums, and coalitions, PPAF activists begin by
listening. Listening involves a mutual relationship between the storyteller and the listener, and
gives the storyteller, often an individual who has been marginalized and oppressed and denied
autonomy, power and agency. In this communicative process, each person “can tell her story
with equal authority, the stories have equal value” (Young 1997:73). Rather than accept only
some stories, PPAF engages with each story, recognizing that each of their patients has lived
experiences of racism, sexism, and more, and none of these stories is worth more than the others.
The plurality of perspectives enables PPAF to better understand shared experiences, as well as
unshared meanings (Young 1997).
Because PPAF lobbyists have at least some power in the legislature, even if that power is
deeply limited in red states, they can bring those stories to policy-makers, bringing humanity and
dignity into policies that too often take certain bodies for granted. Policies such as the Trans-
Vaginal Ultrasound bill fail to account for the diverse ways in which women’s bodies have
historically been subjugated and ignore the potential for traumatizing and re-traumatizing those
same bodies that the bill purports to serve. PPAF brings their patients’ stories into a policy world
that would otherwise deny certain bodies, certain people agency, and center those stories in their
activist work.
Planned Parenthood, in their (c)(3)’s, (c)(4)’s, and health centers, exists to serve their
patients. They are currently doing this as both a continuation of their history and as an intentional

!
48
divergence. They continue to provide the same quality reproductive and health services that they
have for the past 101 years, refusing to close their doors despite the many attacks they face.
However, they are centering patients and communities they serve in a way that Planned
Parenthood historically failed to do. They elevate their patient’s voices and needs, and do the
essential work of listening. The three legs of the “Planned Parenthood stool”
21
exist for the
primary purpose of serving their patients, and each leg is necessary for Planned Parenthood to
continue to do this work.
CONCLUSIONS AND DISCUSSION
As Planned Parenthood pursues a mission to center the voices and needs of their patients,
different affiliates have mixed ability and results based on the state or local political openness
and atmosphere. I chose to examine two politically distinct states so that I could determine how
this political environment impacted PPAF’s ability to engage with issues of intersectionality and
pursue a reproductive justice agenda.
In the blue state, PPAF is able to focus on far wider and diverse issues and work on
coalitions with more organizations. This is largely because of the sympathetic legislature in that
state. As Blue Past 2 notes, they could get legislators – even moderate democrats – to speak up
for abortion access in the House, so Planned Parenthood didn’t need to be focusing their
resources and energy on that specific reproductive right. Instead, in the blue state, PPAF has
been able to propose broader, reproductive justice oriented legislation by working in coalitions
and engaging with the intersectional issues that their coalition partners see as priorities. In
addition, Planned Parenthood does not face so many attacks in the blue state, so they can propose
proactive legislation and work to expand rather than protect their mission.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
21
The three legs are: health care, education, and advocacy.

!
49
In the red state, the activists I interviewed spoke of wanting to pursue proactive
legislation and expand their mission. However, in the face of a hostile legislature and political
environment, they are constantly on the defensive. The individuals I interviewed from this state
all mentioned the constant negative, restrictive legislation that they had to fight against. In every
legislative session (described by my interviewees) PPAF had to fight at least one bill designed to
limit access to abortion or access to Planned Parenthood, specifically. Because of these attacks,
PPAF has to commit many resources to fighting to protect the limited rights that their patients
have in that state. In addition, the legislative process in this state acts as an additional barrier to
PPAF in the legislature. Specifically, by limiting who can propose legislation and extending the
process of how a bill becomes a law, the legislature has more opportunities to stop PPAF’s
proactive bills, so PPAF has to fight harder here than in most other states just to get a bill onto
the House floor. Although this limits the decisions PPAF can make with their mission in mind,
even in the face of hostility and constraints PPAF is insistent in their broad coalition work and
continues to center their patients to better serve their needs.
Another component of the political opportunity structure in these two states is the
presence of other progressive organizations that PPAF can form coalitions with. In the blue state,
in part because of the overall progressiveness and in part because of the demographic makeup of
the state, there are many other progressive organizations focused on various causes at any given
time. Thus PPAF can be selective in whom they partner with and how they work with those
partners. They can make decisions specifically with the intention of engaging, for example, with
racial justice causes in line with their mission to be more focused on reproductive justice. In the
red state, though, the number of other progressive organizations is limited (in most areas
22
). They
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
22
Red Past 1 noted that, where she was working, “there’s something like 86 non-profits just in
that small location and so people who are activists in general for various issues usually pick their

!
50
also have to be careful with who they partner with because each organization in a coalition could
face political or public backlash for partnering with the others.
However, in both states, PPAF seems to have a great deal of success in sustaining
coalitions. Specifically, because of their professional structure, PPAF can pay activists, such as
the Public Affairs Managers, to sit on coalition tables. This includes meeting with representatives
from other coalition partners, discussing the “issues that are kind of bubbling up for them” (Red
PAM), and setting agendas. In the blue state, this continual engagement enables PPAF to engage
with multiple issues, multiple bills, and multiple candidates at any given time. In the red state,
this continual engagement enables PPAF to do the slow, intentional work that they must do in
order to propose legislation, pass legislation, and get candidates elected. One example of this is
PPAF’s work with Add the Words. The campaign to add the words “gender identity and sexual
orientation” to the state’s nondiscrimination policy has been active for almost 10 years, and by
sustaining that coalition, these two progressive organizations can see progress and pool their
resources to meet the small goals they set in the process of passing this piece of legislation in
such a red state.
Finally, the political environment of each state influence how many resources progressive
organizations can access and how they might deploy those resources in their activism. In the blue
state, PPAF is well funded, has a large volunteer base, and is well respected throughout the state.
Resources in that state are not so scarce, so progressive organizations do not have to fight for
precious funds or volunteers, and instead can pool their resources to reach greater successes than
they could alone. In the red state, though, resources are scarce for progressive organizations.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
top one or two issues and they would already be volunteering on those boards and they just
couldn’t split their time between all 10 issues that are super important to them.” This limited
Planned Parenthood’s volunteer base in that area, as well as their ability to form lasting
coalitions.

!
51
Although PPAF is still well funded, they have to commit those funds primarily to fighting
negative legislation. In addition, volunteers are limited because there are fewer people in the
state who support progressive causes and those who do often work with the organizations
focused on the causes that are most important to them. Similarly, PPAF partners with many
groups from this state because resources are so scarce and progressive groups have to pool their
resources to get anything done in such a hostile state.
Reproductive Justice: From Margin to Center?
Planned Parenthood, in both of the states in my analysis, faces political constraints and
has to set goals that make sense for their particular state. In each, Planned Parenthood has made
strides to consider the intersectional oppression that their patients face by forming coalitions with
groups beyond their normal cohort
23
and by adjusting their mission and how they work toward
that mission. This coalition work, especially, shows the extent to which Planned Parenthood has
moved intersectional politics from the margins to the center of their advocacy. By this, I mean
that Planned Parenthood is centering, focusing on, advocating for precisely those patients who
experience intersectional oppression and structures. According to bell hooks, bringing
communities from margins to center occurs when “the experiences of people on the margin who
suffer sexist oppression and other forms of group oppression are understood, addressed, and
incorporated” (2000:163). Planned Parenthood is doing this essential work in their coalition
work, as they seek to dismantle various intersectional structures of dominance, and in the issues
they pursue they are determined to sustain and enhance their patients’ agency, especially in their
reproductive health.
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
23
The three groups that PPAF partners with consistently and nationally are: ACLU, NOW, and
NARAL.
!
52
Because they are, at the core, a health care provider, PPAF’s activism is largely related to
that central tenant of the organization: protecting health care access, expanding access,
decreasing costs, increasing choice. These issues are not distinct from reproductive justice, and
Planned Parenthood is integrating justice into their activism and their work. They recognize that
they exist to serve their patients, and Planned Parenthood’s commitment to be “centered around
[their] patients” has been both the starting point for their reproductive justice work as well as a
guiding principle for how to continue this work. Centering their patients, centering their stories,
is a long process that requires that Planned Parenthood listen to those stories and be open to
learning from their patients. The activists I interviewed, especially the two current activists, were
willing to do this slow and intentional work, were engaging with justice causes in their
legislative work, advocacy, and health care provision. To be attentive to their history is to
recognize what changes they have made; to center their patients is to determine how they must
continue to center reproductive justice; to keep their doors open they must do both, “because at
the end of the day that’s why Planned Parenthood exists: to serve our patients and serve those
communities” (Red PAM).
Suggestions for Further Research
This research was primarily exploratory. Although I focused on three questions, I learned
much more about Planned Parenthood than the answers to those questions. My research also
raises some important questions. Each of the activists I interviewed from the red state spoke with
some degree of tiredness – tiredness stemming from the hostility and opposition that they
experienced as Planned Parenthood employees and activists in such a politically conservative
state. I am curious to know if Planned Parenthood activists remain with the organization in these
environments. In such a hostile political environment do activists continue to work with PPAF?
!
53
If so, why? Red PAM seemed to do so because of a personal dedication to Planned Parenthood’s
mission, but others might persist because they are responding to a specific need. And for those
who do not remain active overtime, is it a response to the political environment? In addition, the
current Public Affairs Manager has so many duties and tasks in her position because of limited
staffing and funding. I imagine the diversity and quantity of responsibilities would be taxing –
especially when she has to celebrate small victories and can rarely get proactive legislation
passed. Working in a state with limited resources, being constantly under attack would, I think,
be exhausting. I would be interested to see if and why activists continue to work with PPAF in
these conditions.
As mine is the first study to examine Planned Parenthood as an organization, there are so
many other questions, so much more to know about this organization. Planned Parenthood has
engaged in 100 years of health care and activism, has aided in monumental successes for
women’s rights, and has built health centers and provided care for so many. If their doors stay
open, what will be their next chapter? I believe it will be a more intersectional care network,
facilitated through broad coalitions, goal setting, and centering their patients.
!
54
REFERENCES
Ahmed, Sara. 2017. Living a Feminist Life. Durham, NC: Duke University Press.
Andrews, Kenneth T., and Bob Edwards. 2005. “The Organizational Structure of Local
Environmentalism.” Mobilization: An International Journal 10(2):213-234.
Brown, Wendy. “Finding the Man in the State.” Feminist Studies 18(1):7-34.
Butler, Judith. 1988. “Performative Acts and Gender Constitution: An Essay in Phenomenology
and Feminist Theory.” Theater Journal 40(4):519-531.
Butler, Judith. 1990. Gender Trouble: Feminism and the Subversion of Identity. New York:
Rutledge.
Carastathis, Anna. 2013. “Identity Categories as Potential Coalitions.” Signs 38(4):941-965.
Cho, Sumi, Kimberle Crenshaw, and Leslie McCall. 2013. “Toward a Field of Intersectionality
Studies: Theory, Applications, and Praxis.” Signs 38(4):785-810.
Crenshaw, Kimberle. 1991. “Mapping the Margins: Intersectionality, Identity Politics, and
Violence against Women of Color.” Stanford Law Review 43(6):1241-1299.
Davis, Flora. 1991. Moving the Mountain: The Women’s Movement in America since 1960. New
York: Vintage Books.
Edwards, Bob, and John D. McCarthy. 2004. “Resources and Social Movement Mobilization.”
pp. 116-152 in The Blackwell Companion to Social Movements, edited by D. A. Snow, S. A.
Soule, and H. Kriesi. Oxford: Blackwell Publishing.
Ehrenreich, Barbara, and Deirdre English. 2012. “Witches, Midwives, and Nurses: A History of
Women Healers.” In Voices of the Women’s Health Movement (vol. 1), edited by Barbara
Seaman with Laura Eldridge, pp. 6-24. New York: Seven Stories Press.
Freeman, Jo. 1973. “Origins of the Women’s Liberation Movement.” American Journal of
Sociology 78:792-811.
Ganz, Marshall. 2000. “Resources and Resourcefulness: Strategic Capacity in the Unionization
of California Agriculture, 1959-1966.” American Journal of Sociology 105(4):1003-1062.
Goldner, Melinda. 2017. “Women’s Health Social Movements.” In The Oxford Handbook of
U.S. Women’s Social Movement Activism, edited by Holly J. McCammon, Verta Taylor, Jo
Reger, and Rachel L. Einwohner, pp. 254-269. New York: Oxford University Press.
Harnois, Catherine. 2012. “Sociological Research on Feminism and the Women’s Movement:
Ideology, Identity, and Practice.” Sociology Compass 6(10):823-832.
hooks, bell. 2000. Feminist Theory From Margin to Centre. London: Pluto.
Internal Revenue Service. 2018. “Social Welfare Organizations.” Washington, D.C.: Internal
Revenue Service. Retrieved April 16, 2018 (https://www.irs.gov/charities-non-profits/other-
non-profits/social-welfare-organizations).
Klandermans, Bert and Suzanne Staggenborg, eds. 2002. Methods of Social Movement Research.
Minneapolis, MN: University of Minnesota Press.
Kline, Wendy. 2008. “The Making of Our Bodes, Ourselves: Rethinking Women’s Health and
Second-Wave Feminism.” In Feminist Coalitions: Historical Perspectives on Second-Wave
Feminism in the United States, edited by Stephanie Gilmore, pp. 63-83. Urbana: University
of Illinois Press.
Krieger, Nancy and George Davey Smith. 2004. ““Bodies Count,” and Body Counts: Social
Epidemiology and Embodying Inequality.” Epidemiological Reviews 26(1):92-103.
Loyd, Jenna M. Health Rights are Civil Rights: Peace and Justice Activism in Los Angeles 1963-
1978. Minneapolis: University of Minnesota Press.
!
55
Meyer, David S. 2015. The Politics of Protest. New York, NY: Oxford University Press.
Meyer, David S. and Suzanne Staggenborg. 1996. “Movements, Countermovements, and the
Structure of Political Opportunity.” American Journal of Sociology 101(6):1628-1660.
Planned Parenthood Action Fund. 2018. “About Planned Parenthood Action Fund.” Washington,
D.C.: Planned Parenthood Action Fund. Retrieved April 12, 2018
(https://www.plannedparenthoodaction.org/about-us).
Planned Parenthood Federation of America. 2017. “2016-2017 Annual Report.” Washington,
D.C.: Planned Parenthood Federation of America. Retrieved April 18, 2018
(https://www.plannedparenthood.org/about-us/facts-figures/annual-report).
Planned Parenthood Federation of America. 2018a. “Who We Are: Our History.” Washington,
D.C.: Planned Parenthood Federation of America. Retrieved April 24, 2018
(https://www.plannedparenthood.org/about-us/who-we-are/our-history).
Planned Parenthood Federation of America. 2018b. “Who We Are: Mission.” Washington, D.C.:
Planned Parenthood Federation of America. Retrieved April 24, 2018
(https://www.plannedparenthood.org/about-us/who-we-are/mission).
Reger, Jo. 2002. “Organizational Dynamics and Construction of Multiple Feminist Identities in
the National Organization for Women.” Gender & Society 16:710–727.
Reger, Jo. 2017. “Contemporary Feminism and Beyond.” In The Oxford Handbook of U.S.
Women’s Social Movement Activism, edited by Holly J. McCammon, Verta Taylor, Jo Reger,
and Rachel L. Einwohner, pp. 109-128. New York: Oxford University Press.
Reger, Jo and Suzanne Staggenborg. 2006. “Patterns of Mobilization in Local Movement
Organizations: Leadership and Strategy in Four National Organization for Women
Chapters.” Sociological Perspectives 49(3):297-323.
Ruzek, Sheryl Burt. 2012. “Map of the Women’s Health Movement.” In Voices of the Women’s
Health Movement (vol. 2), edited by Barbara Seaman with Laura Eldridge, pp. 308-315. New
York: Seven Stories Press.
Scott, Ellen K. 2005. “Beyond Tokenism: The Making of Racially Diverse Feminist
Organizations.” Social Problems 52(2):232-254.
Showden, Carisa R. 2011. Choices Women Make: Agency in Domestic Violence, Assisted
Reproduction, and Sex Work. Minnesota, MN: University of Minnesota Press.
Staggenborg, Suzanne. 1986. “Coalition Work in the Pro-Choice Movement: Organizational and
Environmental Opportunities and Obstacles.” Social Problems 33(5):374-390.
Staggenborg, Suzanne. 1988. “The Consequences of Professionalization and Formalization in the
Pro-Choice Movement.” American Sociological Review 53(4):585-605.
Staggenborg, Suzanne. 2011. Social Movements. New York, NY: Oxford University Press.
Staggenborg, Suzanne, and Marie B. Skoczylas. 2017. “Battles Over Abortion and Reproductive
Rights: Movement Mobilization and Strategy.” In The Oxford Handbook of U.S. Women’s
Social Movement Activism, edited by Holly J. McCammon, Verta Taylor, Jo Reger, and
Rachel L. Einwohner, pp. 214-231. New York: Oxford University Press.
Tarrow, Sidney. 1998. Power in Movement: Social Movements and Contentious Politics, 2
nd
ed.
Cambridge: Cambridge University Press.
Taylor, Verta. 1989. “Social Movement Continuity: The Women’s Movement in Abeyance.”
American Sociological Review 54:761-75.
Taylor, Verta. 1999. “Gender and Social Movements: Gender Processes in Women’s Self-Help
Movements.” Gender and Society 13:101-119.
!
56
Taylor, Verta, and Lisa Leitz. 2010. “From Infanticide to Activism: Emotions and Identity.” In
Social Movements and the Transformation of American Health Care, edited by Jane C.
Banaszak-Holl, Sandra R. Levitsky, and Mayer N. Zald, pp. 266-283. Oxford: Oxford
University Press.
Threadcraft, Shatema. 2016. Intimate Justice: The Black Female Body and the Body Politic. New
York: Oxford University Press.
Weisman, Carol S. 1998. Women’s Health Care: Activist Traditions and Institutional Change.
Baltimore, MD: Johns Hopkins University Press.
Young, Iris Marion. 1997. Intersecting Voices: Dilemmas of Gender, Political Philosophy, and
Policy. Princeton, NJ: Princeton University Press.

!
57
Appendix A. Interview Questions
Introduction
Thank you for participating in this interview. I will ask you a series of questions related to your
role at Planned Parenthood Votes Northwest, and how this office sets and pursues it’s goals.
These questions fall under six broad sections. The first relate to your personal and professional
background. The second relate to the Action Fund’s structure and functions. The third section
regards the issues your office focuses on. In the fourth section I will ask questions about how
your organization sets and works toward accomplishing its goals. Fifth, I will ask how you frame
or discuss those issues with different audiences. In the last section I will ask about how you
define success and to describe some recent successes.
Before I we begin the interview I am required to ask for your consent to participate in this
interview. I sent you the informed consent form this morning, but just to remind you before we
start, I will not use your real name in my paper, nor will I state the specific office you work for. I
am recording this interview, but I am the only one who will have access to that recording and I
will delete recording and transcript in June when I have completed my senior thesis. Do you
consent and agree to participate in this study?
[CONSENT FORM READ, QUESTIONS ANSWERED, SIGNATURE ACQUIRED]
Thank you for agreeing to this interview. I’d like to start by asking you some basic questions
about your background:
Background Questions
Demographic Questions
a) How old are you?
b) What is your gender identity?
c) What race/ethnicity do you identify as?
Professional Questions
a) How long have you been working for PPAF?
b) What is your position at PPAF?
c) What are your duties/tasks in that position?

!
58
d) What (if any) other positions have you had during your time with this office?
a. How were your responsibilities different in that position?
e) Were you employed before coming to PPAF?
a. If yes: What did your job at _____________ entail?
The next set of questions relate to the structure and functioning of the organization. I have
carefully read your website and I’m seeking more in-depth responses to help me understand your
organization.
Organizational Questions
a) Does your office focus more on local, state, regional, or national issues?
b) What do you think is the main purpose of this office of PPAF specifically?
c) In what capacity does this office work with the national ACTION FUND and
FEDERATION offices?
a. How often do you work with those offices?
d) In what capacity does this office work with the state- and local-level Planned Parenthood
Federation offices?
b. How often do you work with those offices?
e) Are you currently working with any outside organizations? {SISTER SONG?}
c. What projects are you working on with this (these) organization(s)?
d. How long have you been working with those organizations?
e. In what capacity do you work with those organizations?
f. How do you decide which outside organizations to work with?
g. Have you faced any problems in your work with outside organizations? If yes,
could you give me an example?

!
59
The next section includes questions about the issues this office is focusing on. I have closely read
your website, but I’d really like a deeper understanding of the issues you are currently focused
on.
Issue
a) What are the central issues your office is working on right now?
a. Health care reform, birth control/preventative care, sex ed, abortion access,
opposing attacks on women’s health, reproductive justice
b) How does your office decide what issues to focus on at a given time?
We’re about halfway through the interview. Next I will ask some questions about how you create
and work to achieve goals.
Goals & Actions
a) What are some short-term goals you’re currently working toward?
b) What are some long-term goals you’re currently working toward?
c) How does your office decide its short-term goals?
d) How does your office decide its long-term goals?
e) How does your office take consideration of the diverse population in the region you serve
when you make these goals?
f) Does your office create goals with assistance from the national PPAF organization?
a. If yes: how often do you work with the national organization to set your goals?
And: do you work with any other organizations or group besides the national
office? If yes, how do you work with these other organizations?
b. If no: do you work with any other organizations or groups?
And: how do you work with other organizations?

!
60
And: Did you face any difficulties in your work with _____ (name organization)
while setting goals?
g) I noticed that there are Planned Parenthood Action Fund offices at the state- and local-
level in some of the states you serve, such as (example). Do you work with those offices
to set goals? If yes, how?
h) What activities does your group do to reach its short-term goals (e.g., letter writing
campaigns, lobbying)?
i) What activities does your group do to reach its long-term goals (e.g., grow membership,
educational programs)?
j) What were some barriers you faced in attempting to achieve these goals? How did your
branch seek to overcome those barriers?
The next set of questions focus on how you frame or present the issues that you work on to
different audiences.
Framing
a) How do you frame the issues you work on to your members and supporters?
b) How do you frame the issues you work on when trying to gain new supporters?
c) How do you frame the issues you work on when you’re trying to persuade politicians to
support or change legislation?
a. Since this branch serves a large region, how do you frame the issues differently in
the different states you service?
If they need an example, offer two different states in the region.
d) Are there political differences in the states you serve? If so, how do you manage your
message given these political differences?

!
61
a. Do you ever worry that there might be political backlash in one state based on
your actions in another state? If yes, how do you navigate this in your framing or
messaging?
e) Probing question: You mentioned earlier that one of your goals is to reach out to certain
communities, how do you frame your issues with those communities?
We’re almost finished! In this next section I will ask you about how you define success and what
has helped you achieve your goals.
Success Questions
a) How would you define a success for PPAF?
b) What have been some of this branch’s recent successes?
a. Who do you think benefited most from that (state success) success?
c) What specific policy outcomes has this branch of PPAF helped to bring about?
To follow up:
Were there any organizations you worked with to further those successes?
My final questions are:
Closing Questions
a) Is there anything you’d like to add to your answers?
b) Are there any questions you think I should ask but didn’t?
c) Do you have any questions for me?
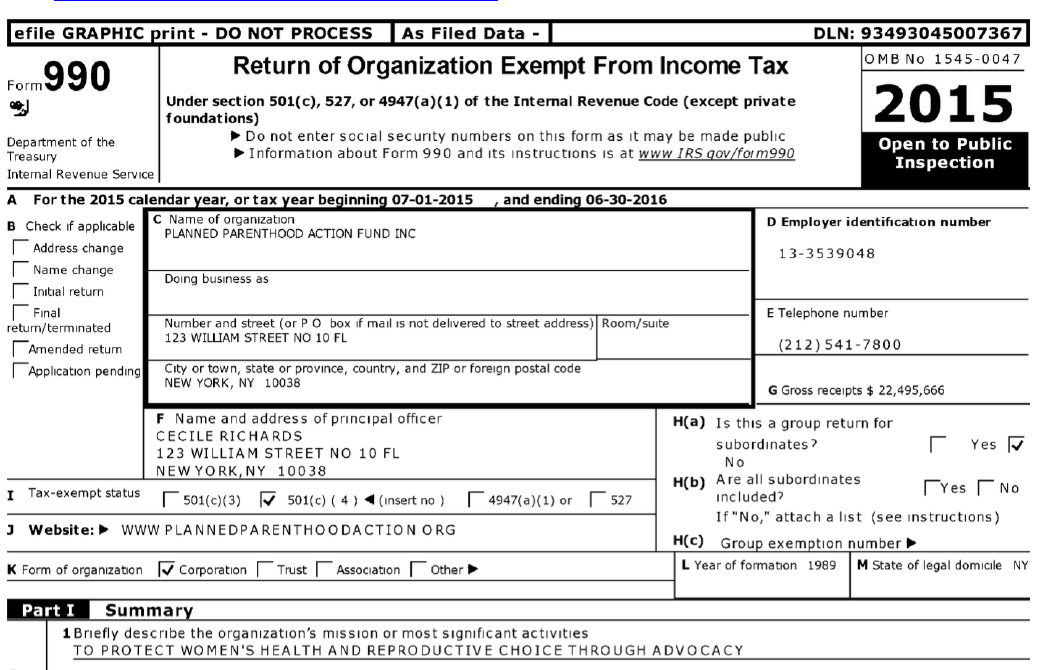
!
62
Appendix B. Archival Data
Planned Parenthood Action Fund
IRS Form 990
Retrieved April 17, 2018
https://www.guidestar.org/profile/13-3539048
!
63
Planned Parenthood Federation of America
IRS Form 990
Retrieved April 17, 2018
https://www.guidestar.org/profile/13-1644147
!
64
Appendix C. Descriptions of Interview Subjects
Office
Time with
Planned
Parenthood
Position(s)
Duties
Level of Focus
Blue PAM
Female
White
State-level PPAF
affiliate
10 years;
2008-present
Public Affairs
Manager
Drive strategy on
all campaigns;
working with
policy team,
communication
team, and field
team; supervisor
of field
organizing team
State; depends on
priority
Blue Past 1
Female
White
Local PPFA affiliate
15 years;
2000-2015
Director of
External Affairs
Fundraising;
Marketing;
limited public
policy work
Local; some state;
some regional and
national
Blue Past 2
Female
White
Regional PPAF
affiliate (housed in blue
state)
2 years;
2011-2013
Communication
Coordinator
Media and press
relations; email
marketing; social
media
management
Regional; depends
on priority
Red PAM
Female
White
State-level PPAF
affiliate
4 years;
2014-present
Legislative
Director and
Public Affairs
Manager
Head lobbyist; set
legislative
priorities; work
with coalition
partners and
progressive
groups; handle
media requests;
oversee field
organizers;
oversee clergy
program in the
state; liaison
between public
affairs and health
centers; electoral
work
State
Red Past 1
Female
Caucasian
Local PPFA affiliate;
State-level PPAF
affiliate
4 years;
2010-2013
Community
Organizer; Field
Organizer
Managing
volunteers;
hosting
community events
Local; State; some
inter-state
cooperation
Red Past 2
Male
White
Local PPFA affiliate;
State-level PPAF
affiliate
6 years;
2004-2009
Field Organizer;
Lobbyist;
Executive
Director (state
PPAF office)
Community
organizing;
fundraising;
tabling; lobbying
Local; State; some
inter-state
cooperation
